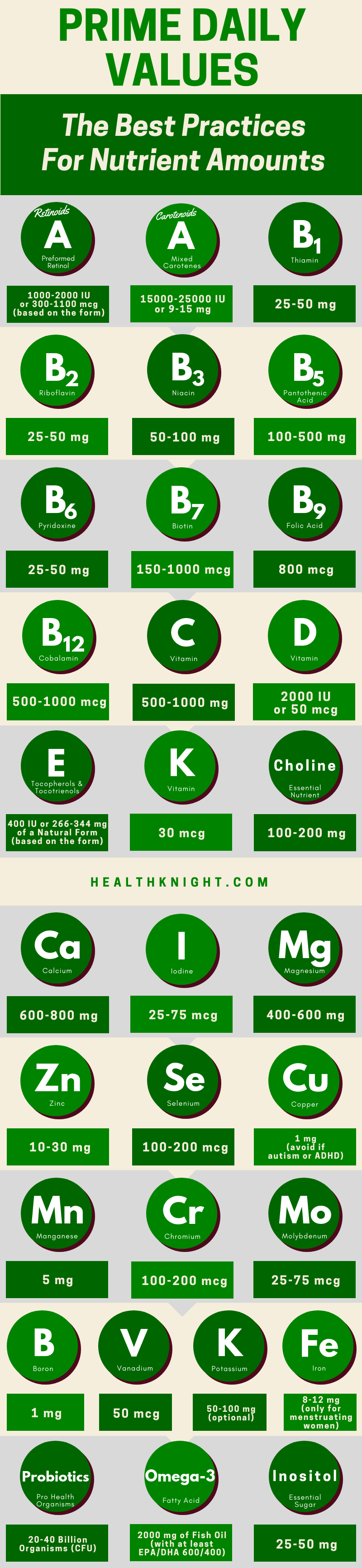
The best practices for nutrient amounts or Prime Daily Values stand for the actual nutrient values that are needed to consume daily with supplements to achieve and retain a state of exceptional health and cognitive ability.
Basically, to be your best self at all times! And to flourish! And thrive! And do so till the rest of your life!
Although I did coin the term Prime Daily Values for easier reference, I did not develop the values themselves. These values have been developed by Dr. Mark Hyman, one of the most respected professionals in medicine, and are published in the book “The UltraMind Solution“.
From what I gather, these values (by now) have been a major factor in helping tens of thousands of people (or likely even more than that) to repair their health, fix and augment their brain, improve their general well-being and life quality.
Over time I have made small insignificant adjustments to these values that are fully based on what other high-profile health professionals recommend and define as the truth. Which I’ll explain all about below.
Amendments Made To The Original Prime Daily Values & Why?
So, as I already mentioned, above you can see infographics of the most up-to-date, amended, and improved Prime Daily Values (the best practices for nutrient amounts).
In the sections to come, I will explain what the changes have been, as well as I will cover what they originally were. So, you have both of the options available to you and you can follow the one whichever seems to reflect the truth to you the most.
Other than that, I want you to know that any future adjustments that we will make to the best practices for nutrient amounts (Prime Daily Values), I will also list here below.
Tocopherols & Tocotrienols Instead Of Mixed Tocopherols (Vitamin E)
Originally Dr. Mark Hyman recommended taking mixed tocopherols (4 different forms of vitamin E) in amounts of 400 IU daily for your best health.

However, I feel these 4 forms do not do justice to vitamin E. Vitamin is much more than 4 different compounds. In truth, it’s about 8 different ones – 4 types of Tocopherols (alpha, beta, gamma, delta) and 4 types of Tocotrienols (alpha, beta, gamma, delta).
Furthermore, as indicated by Andreas M. Papas, Ph.D., and Benjamin V. Treadwell, Ph.D., all of these forms are hugely important, they serve very different functions, moreover, they compliment each other. Thus, all of them contributing to health in their own unique way [R, R, R, R, R, R, R, R, R]
Hence, given that Prime Daily Values, in essence, are about getting to, having, retaining the best health possible, I feel Tocotrienols are something that is a crucial part of all of that and can contribute to anyone’s well-being quite a bit.
That said, supplements actually providing that form of vitamin E are a different story. Mainly because you won’t find them there that often, especially when talking about multivitamin supplements. Still, when you do, it’s something that can only further benefit you.
Potassium Coined As Something Optional Instead Of Something Necessary
Another thing that originally was different about Prime Daily Values was it not listing Potassium as an optional thing. However, I do have a reason to believe that it essentially always has been the case.

Having extra Potassium may superficially seem like a good thing, however, it’s completely unnecessary. In fact, it can easily lead to overdosing on the mineral, which can be lethal and does require immediate medical treatment, as well as there are other concerns [R, R, R, R].
Thus, it makes complete sense that you won’t find any high-profile doctor recommending Potassium supplements as something necessary. Instead, it is said that you are likely to (or if not can) get more than enough from food sources alone. Consequently, Potassium supplements are something you’ll only ever need if under specific medical circumstances [R, R, R, R]
So, why was it included in the Prime Daily Values at all in the first place?
I believe mainly it was due to two reasons. First, a little extra Potassium can’t really hurt. Second, it’s pretty common in many multivitamins.
To illustrate, you should be getting (but many fall below that) up to 4700 mg daily of this mineral. So, 50 or 100 mg extra won’t be exactly the amount that will make or break things [R, R, R, R, R, R, R].
For Omega-3 Fatty Acids, “At Least” Is The Name Of The Game (EPA & DHA)
For Omega-3 fatty acids through Fish Oil, originally Dr. Mark Hyman recommended 1000 mg that consists of 300 mg of EPA and 200 mg of DHA twice daily. However, there’s a very high chance of this being an “at least amount”.

The reason for this lies in the incredible beneficialness of Omega-3 fatty acids (especially on brain-function), as well as the fact that you can get way more out of them if you do go with higher concentrations.
Both studies and other high-profile health professionals agree on this [R, R, R, R, R, R, R, R, R].
That said, don’t get me wrong. I’m not trying to imply that 2000 mg of fish oil with combined amounts of 1000 mg EPA & DHA daily is insufficient for great health. Not at all. It’s likely more than enough.
However, we’re after the truth. And the truth at this moment seems to be that by adding a little bit more (for example, combined amounts of 1200 mg EPA & DHA daily) you can get some extra more out of it.
Why Prime Daily Values Over DV, NRV, Or Any Similar Values?
These values, which you typically see labeled on the supplements (and which indicate a percentage of any respective nutrient that you get), are based on an outdated model. Per the teachings of Dr. Mark Hyman, a model of deficiency [R].
The key questions within this old model to establish reference values, such as DV (US), NRV (European Union, Australia), or any other similar values, are as follows:
- How much vitamin A is needed to avoid night blindness?
- How much vitamin B1 is needed to avoid beriberi?
- How much vitamin B2 is needed to avoid dermatitis or anemia?
- etc. [R, R, R, R, R, R, R, R, R, R, R, R, R, R, R].
So, what do you think? How much do you need a particular vitamin or mineral (including trace elements) in order to not develop a disease?
Well, typically not very much, which is also what we see, if we take a look at 100% values of DV, NRV, or any other similar value [R].
According to this model, as long as you don’t have any of the deficiency diseases, you are getting enough nutrients (vitamins, minerals, trace elements). But this is simply not true.
You are getting enough nutrients to avoid deficiencies, yes. But not enough to optimize all of your cellular functions (and get the full benefit). Or, in other words, to achieve the best health and cognitive ability possible [R].
To better explain what I mean let’s look at some examples.

In this picture above you can see a hypothetical example of the Magnesium functions in the body. Hypothetical, because there are over 600 functions Magnesium is associated with. But here we have only four (so to say few of the big ones) in the picture [R, R]
So, what happens when one consumes nutrients only in the amounts of minimum daily values (100% of DV, NRV, or any other similar value)? Well, you get the picture below.

Meaning there is enough of Magnesium to ensure that you do not get sick with Hyperexcitability. It probably ensures that you don’t get cramps too. It also prevents other deficiency-induced effects.
But there is too little Magnesium to enhance your memory and ensure great learning ability. And you might think that you’re a slow learner or you have poor memory. Which is not necessarily the case. And all that it really might be, is not having enough Magnesium.
And this doesn’t stop there. Most of these 600 functions will not be carried out effectively or at all, because of the fact that your body simply does not have enough Magnesium.
Let’s look at another example.

Similarly, as with the Magnesium, also Vitamin D carries out quite a bit different functions in the body. For the sake of example, we have 3 of them in the picture (we’ll keep sticking with the few of the big ones for simplicity) [R, R].
Well, what happens when one consumes only the minimum daily values of nutrients (100% of DV, NRV, or any other similar value)? Similarly, as with Magnesium, you get the picture below.

Meaning, you may acquire enough Vitamin D to prevent rickets. But as all of it goes towards that goal, you might be hit by feeling constantly tired or getting sick (colds and bronchitis through the roof) [R, R, R, R].
Furthermore, nutrient deficiencies can also develop so-called long-latency diseases. These diseases happen when for a long period of time (many, many years) there is not enough of a particular nutrient for optimal cellular function. But DV, NRV, and other similar values do not ensure optimal cellular function [R].
For example, not having enough Folic Acid (being seriously deficient) in a pretty short time will develop amenia or birth defects for a baby. But in the long run, having not enough of the nutrient for optimal cellular function has a significantly higher chance of developing Alzheimer’s disease [R].
Other long-latency diseases include schizophrenia, attention-deficit disorder, cancer, depression, heart disease, dementia, and many other [R].
Thus, because all of this, being conservative and consuming nutrients only according to DV, NRV, or other similar values over the long run won’t ensure that you don’t develop these hugely devastating diseases and conditions mentioned.
Why Daily Values Are So Low When The Tolerable Upper Intake Levels Are So High?
If the ideas discussed before did not convince you, consider the following.
If you’ve ever come across the Tolerable Upper Intake Levels (ULs for short) – have you ever thought about why these established DV, NRV, and other similar values are so low, but the ULs are so high?
“What is a UL (Tolerable Upper Intake Level)?” you might ask.
Well, simply put, those are levels set to formulate the highest amount of a particular nutrient intake daily that poses no risk of adverse effects when used for very, very, very long periods of time. To put it in other words, if you do not exceed these levels formulated, there is no risk of acquiring a disease or an adverse condition of some kind [R, R].
Of course, risk-wise ULs are referable to 98-99% of the population. We all are different. So it is possible that for 1-2% of the population these levels can be lower or even higher.
To better understand where I’m going with this, let’s look at an example of DV and NRV in respect to the established ULs, shall we?

NRV and DV values for Vitamin E are 12 mg and 30 IU, respectively.
UL for European Union is 300 mg, therefore, the gap between the respective NRV and its UL is 288 mg. UL for the US, on the other hand, is 1000 mg, therefore, there is a gap of at least 970 mg.

Take a minute and just really let that sink in!
288 mg gap, when no adverse effects of using Vitamin E are present! That’s 24 times the NRV value. Or about 39 times the DV value in the case with that ridiculous 970 mg difference for the US.
I mean, at this point, I feel it’s fair to point out that there must be a reasonable explanation to this. Because can you deny the huge gap and explain it with “oh, I just peed out everything because my body didn’t need that 300-ish mg or 400 IU of vitamin E”?
I believe not. And this is exactly my point.
Many will still try to. Many will justify the situation with the classical: “Yes, this can be easily explained because most probably any excess Vitamin E will easily be excreted from the body. 300 mg or 1000 mg probably is just too much of the amount, which our bodies can no longer reliably excrete.”
While it superficially may seem like a solid point. It’s not one.
Vitamin E is a fat-soluble vitamin. And being fat-soluble, it’s not really known for its easy excretion from the body because no fat-soluble vitamin is that when consumed in excess amounts. This unique ability can only be allocated to the water-soluble vitamins [R, R, R, R].

Thus, a consequential question arises. Where do these amounts of either 300 mg (EU) or 1000 mg (US) go?
Where do they go, if this amount can be consumed for years in and years out without posing any threat or adverse effects to health?
There is only a single reasonable explanation for this. This previously thought excess vitamin E actually gets utilized by the body to carry out important functions (which, of course, it doesn’t do when the amounts of the vitamin are scarce).
Moreover, if we were to look at other vitamins and minerals and their respective UL values, we would encounter similar gaps to those already discussed most of the time. They may at times not be so huge, but they are there.
Which may raise the question of “why only most of the time”?
Why At Times DV Are Higher Than Prime Daily Values (The Best Practices)?
Yes, at times DV, NRV, or any other similar type of value is higher than that mentioned by the Prime Daily Values. “Why is that” is such an awesome and attentive question.
Here’s why.
") The difference lies in what these two types of values stand for.
The difference lies in what these two types of values stand for.
Meaning, DV, NRV, and similar value focus on minimal daily requirements for nutrients that you need to consume. And do so in any way – food, supplements, drinks, shakes, anything else that’s edible.
Whereas Prime Daily Values stand for, as indicated at the very beginning of this article, the actual nutrient values that are needed to consume daily with supplements (and with supplements only) for great health.
Thus, these do not account for all sources of the nutrients (vitamins and minerals) as the DV, NRV, and similar values do.
Hence, the difference.
At the end of the day, still, I don’t hope that everyone will understand this. Or be flexible enough to see that maybe there’s a different truth out there than that what they have been convinced of in the past.
Remember that “convictions are greater enemies to truth than lies” (a quote by Nietzche). Don’t be a person, who’s misguided by one’s own convictions if you have any.
I know, it takes a level of open-mindedness and faith in a guy without a Ph.D. or MD (if we don’t account for his initials). But I’m all about the truth (and research), I can promise you that.
And if it helps at all, know that I took the very essence of these ideas from one of the most respected doctors in the field all of (functional) medicine – Dr. Mark Hyman.
This article was originally published on November 4, 2017. The article was republished on July 19, 2019.
Sorry for the double post. I forgot to ask you about essential minerals like Iron and Copper that usually are absent or in very low quantities in multivitamins.
Dairy is very very low in both of them, not even getting 10% of the RDA with a 2000-2500 calorie diet.
Is it worth to get them from another supplements? I am worried because low iron equals low energy, anemia. And copper helps iron metabolization, so I am worried that even if I get an Iron supplement, without Copper would not be too effective.
My diet right now have 1.5 mg of Iron daily (8 mg RDA for men) but I think calcium affect absorption of it, so may be even less. And 0.2 mg of Copper (0.9 mg RDA).
And with that being said, do you know about any other important mineral or vitamin that usually multivitamins don’t have (like Iron) or only have in very low quantities, usually less than the RDA? (like Copper)
Thank you very much!
Hey, again, Kryzpo!
I feel you. And I absolutely love your awareness on all this.
Generally speaking, as I see it, Iron supplements or just Iron in general is a pretty bad idea for men long-term. However, as far as I can tell from what you’ve shared, in your specific case, it makes a lot of sense (it commonly also makes sense for people with other dietary restrictions; vegan is just one example). I have some real great ones listed on the very best multivitamin list in the section on how to make any supplement great for women. On that note, taking that once every other day should probably work best.
As for the necessary minerals and vitamins commonly low in multivitamins, that’s an incredibly broad question. I mean, with the best of the very best multivitamins we won’t ever have that problem. And those don’t have Iron because of the specific criteria I based that list around.
But other than that, I’ve seen all kinds of things. Supplements struggling with Selenium, supplements strongly lacking in Chromium, supplements offering such unnecessary (borderline harmful) minerals to supplement like Nickel, supplements that use Copper forms that are known to be completely unabsorbable for our bodies, supplements ignoring Boron, Vanadium, or Molybdenum (extremely common), supplement overdoing Potassium, supplements forgetting Iodine. I mean, there’s just every kind of thing out there.
Additionally, as far as I’m aware, vitamin C also plays a huge role in the Iron absorption. So, in the light of what I mentioned in the answer on your previous comment, to the very least picking a multivitamin plus Iron – it’s what I would do if I was on such dietary restrictions as you are.
But be that as it may, I want to thank you, Kryzpo! Speaking with you has actually inspired me to consider starting a new section of articles. The way I see it, it would be awesome to properly research all of these vitamin and mineral interactions to learn and know for sure what influences what, and what is necessary for what, and really bring light into how it all works together.
I appreciate you, man! Cheers,
Matiss
Hi again!
I wanted to ask about what do you think about going higher on some vitamins/minerals. For example, in Vitamin A retinol you have 1000-2000IU daily for ideal intake. About that, what do you think of intakes up to 10.000 IU daily long term?
I ask because I read an article about Sweden women and men who were more likely to hip fractures with 6k or higher Vitamin A retinol intake. I assume that they were getting high vitamin A intakes because dairy consumption. Because that they surely had high calcium levels aswell, but even with that, they have a somewhat lower bone health than people consuming low/moderate Vitamin A retinol. The difference was not too high on those studys though. If I remember well, the risk was like 10-20% more compared to low/moderate Vitamin A retinol consumption.
About this, would be the reason, perhaps, being Sweden, that they probably had low Vitamin D status? and, I am theorizing here, but, perhaps, if you consume high vitamin A retinol, you would need higher intakes of Vitamin D too? being the two relate in bone health. And also, a second theory, if you have high calcium intakes, do you need also higher Vitamin K intakes? or at least adequate intakes of Vitamin D and K?
About that last theory (higher intakes of Vitamin K needed if high calcium intakes), why only 30mcg, lower than the RDA? (90-120mcg)
I want to share this study: https://academic.oup.com/ajcn/article/69/4/656/4737355
In that study people consuming ~20.000 IU Vitamin A retinol daily for 12 years did not shown toxicity levels, so we can perhaps discard that the Sweden study was a consequence of symptoms of toxicity.
Sorry for the long post, but because allergens and other problems, I am consuming a very monotone diet, being this 90% dairy every day. This is because I can tolerate dairy just fine, and being dairy calorie dense (cheese, heavy cream, etc.) I can exercise and get my TDEE or surplus calorie intake more easily without disrupting my stomach.
Thank you!
Hey, Kryzpo!
I just want to thank you for bringing my attention to that 12-year study. I believe it’s so relevant. Whereas as for that Swedish study, I definitely agree. 10-20% is not a lot. So, it might not be that applicable overall.
As for the vitamin D levels in that regard, I’m not too familiar with the notion but I reckon that might, indeed, be the case. Also, just theorizing here. Other than that, if I’m not mistaken, one of the most important functions for vitamin K is that of Calcium deposition. Hence, it might be that both play a role here.
Prime Daily Values represent how much we need with supplements specifically (RDA is more about all sources combined). PDVs are kind of the values that take into account and build on a proper diet. Which, in case, people are aware they are not following, it’s very likely they should go for more. But whatever the case, multivitamins typically still contain more than those 30 mcg.
As for vitamin A amounts, generally speaking, I believe long-term intakes of 10,000 IU should be fine (probably more than fine). Especially, given that Upper Tolerable Intake Levels define that the kind of amounts should not pose any threat to health for 99% of people even if consumed long-term. Both US ones and the EU ones agree on this. And they are usually quite careful about setting them (like often too careful). But with that study you referenced in mind, I’d say that there seems to be a lot more room for vitamin A after all.
And this, as I see it, at least somewhat emphasizes the idea I’ve spoken of before. Meaning, Upper Tolerable Intake Levels apply only if we’re consuming that one vitamin or mineral in very high amounts (because that is how they determine those). If we do that for all of the necessary ones, there is no telling whether such high values that at some point actually become detrimental exist. For all we know, there may not be such a thing.
Above all, I totally feel where you’re coming from. No worries but sorry for my massive delay on the response. Keeping up with the posting commitments are taking their toll on me.
Cheers, and have a Great One!
Matiss
Goodness. You are like me. Very few people like us out there, constantly, fervently, seeking truth with open mind, but not too open that we get deluded. Look forward to more from you. I’ll be taking your multi-vitamin recommendation.
P.S. – My website isn’t setup yet.
Hey, Andrew!
That’s awesome to hear. I’m always happy to meet like-minded people. And you’re absolutely right, there is a danger there one must be very careful about.
Get that website started, mate. It won’t gonna build itself. And let me know if at any point there’s anything I can assist you with. I’ll be happy to hear from you, Andrew!
Cheers, and have a Great One!
Carpe minutam/Seize the moment,
Matiss
Hello, thank you for taking the time to investigate and write these articles, I am looking for a good multivitamin but I still have doubts, should I choose this approach (high doses) or the conventional one?
There are things that make me doubt.
What do you think about this study?
And many others that connect high doses of Vitamin E to bad outcomes?
Also, I read another study some time ago about high doses of Vitamin B12 and B6 linked to lung cancer in men.
Hey, Kryzpo!
This is barely surprising. Many top-level scientists, including Andreas Papas, PhD, (who’s life’s work is on vitamin E and it’s many forms, safety, and all other aspects imaginable) already more than two decades warn that the only vitamin E that you should ever take is one that is of a natural form. Mainly, because the synthetic form of it (that’s, by the way, something still widely used in supplements) is an extremely toxic one even in doses higher than 30 IU.
Don’t quote me on that number though. It might have been something slightly higher but I remember it being something ridiculously low, something barely over 100% DV at the time. Whereas there’s no such thing happening with the natural vitamin E form (d- form).
Thus, if that meta-analysis analyzes studies that have used the synthetic (dl- form) of vitamin E, if anything, the findings make absolute sense.
So, it took me a while but I went through all of the studies analyzed in that meta-analysis you cited.
And in a few words, it’s a fascinatingly confusing study.
In essence, the meta-analysis analyzes 19 studies to conclude that 400 IU/day or more may be causing higher mortality rates. And in that, it divides all of them into two big groups. Those that prove that vitamin E is beneficial and those in which the vitamin is (somewhat) proved to be harmful [R].
So, what about that group of studies that report the vitamin E being harmful?
Most of them pay zero attention to what kind of vitamin E was used. Meaning, not only they don’t pay any attention to the vitamin form in the meta-analysis but also the studies themselves often don’t specify it.
Essentially, I feel the study you cited fails to recognize the massive differences between these two forms of vitamin E. Which is a beyond incredible flaw to it. And thus, I feel is a fool’s game to trust it.
But here things get really interesting (and massively confusing).
While dividing all of those studies in ones that prove either harmfulness or harmlessness, the meta-analysis is extremely inconsistent.
What I mean is that they report certain studies proving that vitamin E is harmful but when you look at the study in full, it says or concludes no such thing.
For example, there was a study that was abbreviated SPACE. The meta-analysis listed it as one that proves that vitamin E improves mortality rates. But the actual study actually concludes that vitamin E, if anything, improves life-span instead of supposedly shortening it (vitamin E form not mentioned).
Or a study (abbreviated VECAT) that hammers down the point about natural vitamin E. Again, the meta-analysis says that this proves vitamin E harmfulness. However, the actual study notes that in their findings there was zero difference in mortality rated between those that took 500 IU natural vitamin E form daily for 4 years and those that didn’t.
Ultimately, I feel the title of the study is exactly what they conclude: “Meta-Analysis: High-Dosage Vitamin E Supplementation May Increase All-Cause Mortality.”
Not “increases”, not “is increasing”, not “proves”, as well as no other form of convincing evidence. Only “may”, which signifies the fact that it may or (way more likely) may not be true. And which ultimately may be just a poor attempt at creating sensationalism, moreover, as I’ve never seen any top-level doctor (14 years have passed since the study was published) talk about this study in relation to proving vitamin E should be avoided (or when considering vitamin E supplementation).
Maybe there’s something I’m missing completely or something that I’m unintentionally ignorant about in which case you are very welcome to add as I’m all about the truth.
But as far as I can tell, to me, this does not seem convincing at all.
Whereas if you still find yourself fluctuating on this and want to supposedly be on the safe side, just make sure that you go below 400 IU of vitamin E (and always that it’s a natural one).
As for the many other studies that connect high doses of vitamin E to bad outcomes, I’m willing to bet my head on the fact that there are way more studies out there that prove vitamin E beneficialness.
As for that study on B6 and B12, as Theodore Brasky, PhD, (author of the study) himself explained, the takeaway message is that the risk of lung cancer may increase substantially in men who smoke and use these kinds of supplements (no such thing in men who don’t or in women in general) [R, R].
However, he did note that the study proves association and not causation. Meaning, while it seems that men smokers may be negatively impacted by B6 and B12 supplementation in terms of lung cancer, there’s no way of telling what kind of other factors contributed to the result.
This is because as an observational study (which this was), it doesn’t account for all the inevitable and often impossible to measure factors, aspects, and exposures that may actually be contributing to and ultimately, causing the results. Hence, not without a reason in the scientific community, such studies often are regarded as speculative at best.
(Or to put it in yet another words, when a study finds an association between two things it does not mean that one thing caused the other to happen.)
So, where does this leave us?
While there may be something there and I’m absolutely willing to look into this more closely when there’s more research available, I don’t feel it’s a proper enough basis at this time to change my own approach to supplementation or the Prime Daily Values in general.
You may feel different about it and that’s okay. We all are different in what kind of nutrients we need physiologically (Prime Daily Values is just a general guideline). Do whatever feels most appropriate to you, Kryzpo. Or try both approaches.
And see which fits you more.
Cheers, and have a Great One!
Carpe minutam/Seize the moment,
Matiss
P. S. Given the length of the comment I might post it as a separate article in category Purely-Opinion not far down the line.